

and
IRIS PROGRAMME
IRIS is a specialist domestic violence and abuse(DVA) training, support and referral programme for general practices that has been positively evaluated in a randomised controlled trial. It is a partnership between health and the specialist DVA sector. IRIS is a specialist domestic violence and abuse(DVA) training.

AANCHAL AND IRIS PROGRAMME
IRIS is a specialist domestic violence and abuse(DVA) training, support and referral programme for general practices that has been positively evaluated in a randomised controlled trial. It is a partnership between health and the specialist DVA sector.
IRIS
IMPROVING THE GENERAL PRACTICE RESPONSE TO DOMESTIC VIOLENCE AND ABUSE
Identification & Referral to improve safety
The IRIS programme can support
your practice and your patients


What is
IRIS
IRIS provides in-house DVA training for general practice teams and a named advocate to whom patients can be referred for support. Since 2010, IRIS has received 10,369 referrals and fully trained an estimated 695 general practices in 36 localities nationwide.
Behind every one of these referrals is a woman being
provided with validation of her experiences and a safe space
to articulate what is happening to her.
provided with validation of her experiences and a safe space
to articulate what is happening to her.
The reality in general practice...
.
.
1/4
One in four women will experience domestic abuse in their life time. Between 6% and 23% of women attending general practice will have experienced physical or sexual abuse from their partner or a previous partner in the preceding year. On average, two women in England and Wales are killed by a male partner or ex-partner each week. (The Health Foundation, 2011. Home Office, 2005)
80%
Eighty percent of women in a violent relationship seek help from health services at least once (usually general practice) and this may be their first or only contact with professionals. (Department of Health, 2000)
15%
Domestic violence is a common problem that is almost invisible in primary healthcare, even though women would most like to receive support from their doctors. Only around 15% of women with a history of domestic violence have any reference to abuse in their medical record in primary care. (Richardson et al, 2002)
The IRIS Model
IRIS provides in-house DVA training for general practice teams and a named advocate to whom patients can be referred for support
INPUTS
Training and
on-going
support
on-going
support
Care
pathways
including
safeguarding
children &
adults
pathways
including
safeguarding
children &
adults
Medical
record
prompts
(HARKS)
record
prompts
(HARKS)
Recording
and flagging
system
and flagging
system
Practice
champion
champion
Health
education
materials
education
materials
Clinical inquiry
Validation
Documentation
Immediate risk
assessment
assessment
Advocate
educator
educator
OUTPUTS
Identification
Referral
Emotional &
practical
support
practical
support
Evaluation &
monitoring
monitoring
OUTCOMES
PATIENTS
Improved
quality of life
Improved
quality of life
Improved
physical &
mental
health
physical &
mental
health
Reduction in
abuse
abuse
PRIMARY CARE
PROFESSIONALS
Improved DVA
response
PROFESSIONALS
Improved DVA
response
Provision of
holistic care
holistic care
Continued
professional
development
professional
development
PRACTICES
DVA aware &
resourced
DVA aware &
resourced
75% of cases of domestic
violence result in
physical injury or mental
health consequences
to women.
(Department of Health,
2005)
violence result in
physical injury or mental
health consequences
to women.
(Department of Health,
2005)
The advocate educator
- The model rests on one Full-time advocate educator working with up to 25 practices.
- The advocate educator is a Specialist DVA worker who is linked to the practices and based in a local specialist DVA service.
- The advocate educator provides training to the practice teams and acts as an ongoing consultant as well as the person to whom they directly refer patients for expert advocacy.
- The advocate educator works in partnership with a local clinical lead to engage with practices and co-deliver training.
How we help
Knowledge and training supports clinicians to recognise domestic violence and abuse.
General practices receive:
In house training for the whole practice
team
team
Clinical team training – Two training sessions, each lasting two hours. Content focuses on how to recognise DVA and how to respond, refer and record disclosures. Administrative team training – One training session, lasting one hour. The training focuses on understanding DVA, responding to patients, resource provision, confidentiality and safety.
Refresher training and additional sessions for new staff are available to all practices.
Refresher training and additional sessions for new staff are available to all practices.
Named contact for patient referrals
Victims and survivors can be referred to the advocate educator. The advocate educator provides emotional and practical support, carries out risk assessments, safety plans and advocates on behalf of the patient as appropriate.
Ongoing support and consultancy
The advocate educator will attend practice meetings quarterly to discuss all aspects of the programme and is available to support the entire practice and individual professionals on a day to day basis by phone, email and when in the practice.
The evidence base for the IRIS model is that it is effective for female patients. However, every practice that is IRIS trained is given a male patient referral pathway so that they will be signposted towards services that support male survivors. Referral pathways for perpetrators of domestic abuse are also provided.
Victims and survivors
attending an IRIS
trained practice are six
times more likely to
be referred to an
advocate.
(Feder et al, 2011)
attending an IRIS
trained practice are six
times more likely to
be referred to an
advocate.
(Feder et al, 2011)
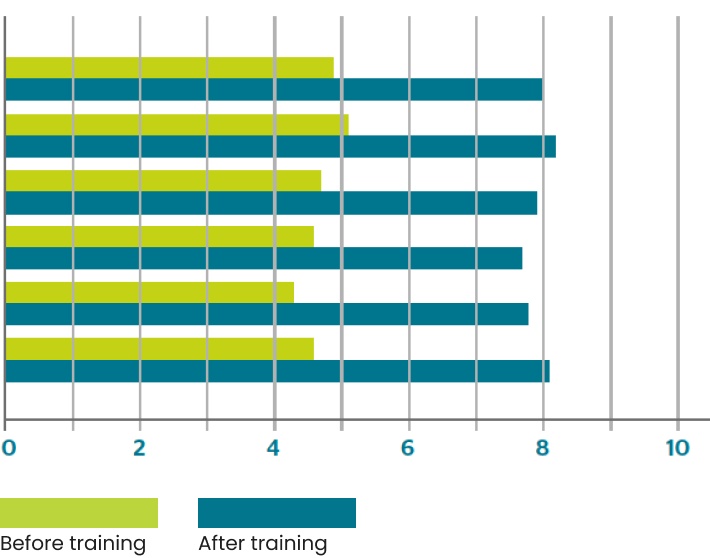
How clinicians feel about IRIS DVA training
What has improved according to
clinicians and general practice staff
Knowledge and skills around DVA
understanding of health consequences around DVA
confidence to deal with and respond to disclosure
ability to assess immediate risk
knowledge of where to refer patients
awareness of support services
understanding of health consequences around DVA
confidence to deal with and respond to disclosure
ability to assess immediate risk
knowledge of where to refer patients
awareness of support services

How does IRIS DVA training benefit you?
“What an excellent
clinical teaching session
– one of the best I’ve
been to in eight years
of medicine”
IRIS trained clinician
clinical teaching session
– one of the best I’ve
been to in eight years
of medicine”
IRIS trained clinician
Ultimately, the whole programme is to the benefit of patients, practices
and practice teams. It:
and practice teams. It:
- Improves safety, quality of life and wellbeing for your patients and their children.
- Provides access to advocacy which benefits victims and survivors of DVA.
- Develops DVA aware practices with fully informed, resourced and equipped practice teams.
- Saves general practices and the wider NHS time and resources.
- Provides holistic care thus achieving better patient outcomes in terms of improved quality of life, physical and mental health and wellbeing.
“I’m now convinced that Violence against Women and Children is a major public health problem with long term consequences for women and their families. As an experienced GP, the whole project has been nothing short of
transformational.” – IRIS GP
transformational.” – IRIS GP
Don’t have enough time for training?
Clinical team training – Two training sessions, each lasting two hours. Content focuses on how to recognise DVA and how to respond, refer and record disclosures. Administrative team training – One training session, lasting one hour. The training focuses on understanding DVA, responding to patients, resource provision, confidentiality and safety.
Refresher training and additional sessions for new staff are available to all practices.
Refresher training and additional sessions for new staff are available to all practices.
How is IRIS different from other DVA referral pathways?
IRIS provides a referral to a named contact, the advocate educator. This referral is made by the clinician, not by the patient, providing a pro-active approach that patients tell us they prefer. Patients can be referred regardless of their level of risk, or whether she wants to leave the relationship or not. Referring clinicians are notified when the advocate educator has received their referral. The practice will also have ongoing support and consultancy, provided by the advocate educator.
What happens to the patient afte they have been referred?
Referring clinicians receive updates from the advocate educator, including information about the support their patient is receiving and other services to which they have been referred. This sharing of information enables monitoring of risk and safety planning.
How does IRIS help your patients?
“Hugely grateful that the Dr
referred me. I wouldn't have
done myself. I was in a very
bad place. I was really lonely
and she didn't push anything
at me, but made it clear
there were options.”
IRIS service user
referred me. I wouldn't have
done myself. I was in a very
bad place. I was really lonely
and she didn't push anything
at me, but made it clear
there were options.”
IRIS service user
Clinical team training consists of two sessions, each lasting two hours. In the long term, this investment of time could save hours of appointment time as 70% of service users report visiting their GP less after being referred to an advocate educator.
Service user outcomes
(IRIS national data report, 2018)
Percentage of service
users that agreed
users that agreed
Pleased to be asked by their clinician
95%
Pleased to be referred to the advocate educator
98%
Felt listened to
99%
Found support helpful
95%
Know where to go for support
97%
Feel safer
86%
Feel more confident
85%
Feel more able to cope
83%
Feel good about myself
95%
Feel optimistic about future
95%
Visit GP less
95%
“I have slowly got my freedom back and
am so happy to be making my own
decisions, planning my own way in life.
This is not just for me, it’s for my children
and women like me out there.”
-IRIS service user
am so happy to be making my own
decisions, planning my own way in life.
This is not just for me, it’s for my children
and women like me out there.”
-IRIS service user
